Can I Give My 1 Year Old Melatonin
[I am non a sleep specialist. Delight consult with one earlier making any drastic changes or trying to treat annihilation serious.]
Van Geiklswijk et al describe supplemental melatonin every bit "a chronobiotic drug with hypnotic backdrop". Using it as a pure hypnotic – a sleeping pill – is similar using an AK-47 as a club to bash your enemies' heads in. It might work, only you're failing to capeesh the full power and subtlety available to you lot.
Melatonin is a neurohormone produced by the pineal gland. In a normal circadian wheel, information technology's everyman (undetectable, less than 1 pg/ml of claret) around the time you wake upward, and stays low throughout the day. Around fifteen hours later on waking, your melatonin of a sudden shoots up to 10 pg/ml – a process chosen "dim low-cal melatonin onset". For the adjacent few hours, melatonin continues to increase, perhaps as high as 60 or 70 pg/ml, making you sleepier and sleepier, and presumably at some point y'all go to bed. Melatonin peaks around 3 AM, then declines until it'southward undetectably depression once more around early morning.
Is this what makes y'all sleepy? Yes and no. Sleepiness is a combination of the circadian bike and the so-called "Process S". This is an unnecessarily sinister-sounding name for the fact that the longer y'all've been awake, the sleepier you'll be. It seems to be partly regulated by a molecule called adenosine. While you lot're awake, the body produces adenosine, which makes you tired; equally you sleep, the trunk clears adenosine away, making y'all feel well-rested over again.
In healthy people these processes work together. Circadian rhythm tells you to experience sleepy at night and awake during the day. Process South tells you to feel awake when you've just risen from sleep (naturally the morning), and tired when you oasis't slept in a long time (naturally the night). Both processes concur that you should experience awake during the day and tired at dark, and then you practise.
When these processes disagree for some reason – nighttime shifts, jet lag, drugs, genetics, playing Civilisation until 5 AM – the arrangement fails. One process tells y'all to go to slumber, the other to wake up. You're never quite awake plenty to feel energized, or quite tired plenty to become restful sleep. You lot find yourself lying in bed tossing and turning, or waking up while it'due south still nighttime and not being able to get dorsum to sleep.
Melatonin works on both systems. It has a weak "hypnotic" effect on Process South, making you immediately sleepier when yous have it. Information technology besides has a stronger "chronobiotic" issue on the circadian rhythm, shifting what time of day your body considers sleep to be a good idea. Effective use of melatonin comes from understanding both these effects and using each where appropriate.
1. Is melatonin an constructive hypnotic?
Yes.
That is, taking melatonin simply before you want to get to slumber, does aid you lot get to sleep. The show on this is pretty unanimous. For primary insomnia, two meta-analyses – one by Brzezinski in 2005 and another by Ferracioli-Oda in 2022 – both notice information technology condom and effective. For jet lag, a meta-analysis by the usually-skeptical Cochrane Collaboration pronounces melatonin "remarkably effective". For a broad range of chief and secondary sleep disorders, Buscemi et al say in their abstract that it doesn't work, but a quick glance at the report shows it absolutely does and they are incorrectly under-reporting their own results. The Psychiatric Times agrees with me on this: "Results from another report reported as negative actually demonstrated a statistically significant positive outcome of a decrease in sleep latency past an average of 7.two minutes for melatonin".
Expert consensus generally follows the meta-analyses: melatonin works. I find cautious endorsements by the Mayo Clinic and John Hopkins less impressive than its less-than-completely-negative review on Science-Based Medicine, a web log I tin usually count on for a striking job on whatever dietary supplement.
The consensus stresses that melatonin is a very weak hypnotic. The Buscemi meta-analysis cites this equally their reason for declaring negative results despite a statistically significant effect – the supplement just made people become to sleep about ten minutes faster. "Ten minutes" sounds pretty pathetic, but we need to recall of this in context. Even the strongest sleep medications, like Ambien, just prove up in studies as getting you lot to sleep ten or twenty minutes faster; this New York Times article says that "viewed every bit a group, [newer sleeping pills similar Ambien, Lunesta, and Sonata] reduced the average time to go to sleep 12.8 minutes compared with faux pills, and increased total sleep fourth dimension 11.4 minutes." I don't know of whatsoever statistically-principled comparison between melatonin and Ambien, but the difference is hardly (pun not intended) solar day and night.
Rather than say "melatonin is crap", I would contend that all sleeping pills take measurable effects that vastly underperform their subjective furnishings. The linked article speculates on one reason this might be: people have low awareness effectually the time they get to sleep, and a lot of people'south perception of whether they're insomniac or not is more anxiety (or sometimes literally dream) than reality. This is possible, simply I as well think of this in terms of antidepressant studies, which find similarly weak objective effects despite patients (and doctors) who swear past them and say they changed their lives. If I had to guess, I would say that the studies include an awkward combination of sick and less-sick people and confuse responders and not-responders. Perhaps this is special pleading. I don't know. But if y'all retrieve whatever sleeping pill works well, melatonin doesn't necessarily work much worse than that.
Slumber latency statistics are hard to compare to one some other considering they're and then dependent on the study population. If your subjects have an hour to fall asleep, perhaps melatonin could shave off thirty-4 minutes. But if your subjects take twenty minutes to fall comatose, so no sleeping pill volition ever take off thirty-four minutes, and even an astonishing sleeping pill might struggle to brand xv. I cannot directly compare the people who say melatonin gives back 10 minutes to the people who say melatonin gives back 30-four minutes to the people who say Ambien gives back twelve, but my totally unprincipled guess is that melatonin is about a third as strong equally Ambien. It also has about a hundred times fewer side effects, so there's definitely a place for it in slumber medicine.
2. What is the right dose of melatonin?
0.3 mg.
"But my local drugstore sells 10 mg pills! When I asked if they had anything lower, they looked through their stockroom and were eventually able to find three mg pills! And yous're saying the correct dose is a third of a milligram?!"
Yes. Most existing melatonin tablets are around ten to thirty times the correct dose.
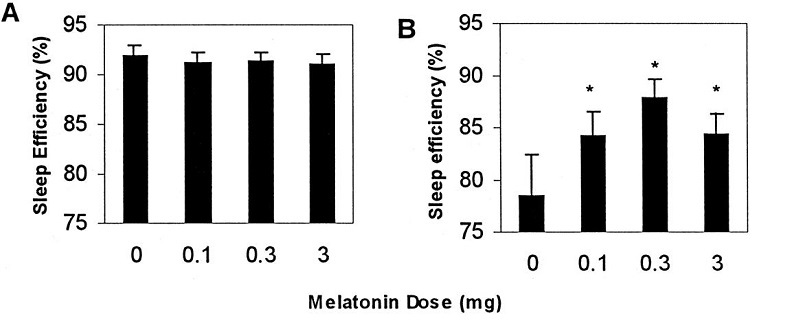
Many early studies were done on elderly people, who produce less endogenous melatonin than young people and and so are considered especially responsive to the drug. Several lines of bear witness determined that 0.iii mg was the best dose for this population. Elderly people given doses around 0.3 mg slept better than those given three mg or more than and had fewer side effects (Zhdanova et al 2001). A meta-analysis of dose-response relationships concurred, finding a plateau issue effectually 0.three mg, with doses after that having no more efficacy, but worse side effects (Brzezinski et al, 2005). And doses around 0.three mg cause blood melatonin spikes well-nigh similar in magnitude and duration to the spikes seen in healthy immature people with normal sleep (Vural et al, 2014).
Other studies were done on blind people, who are especially sensitive to melatonin since they lack light cues to entrain their circadian rhythms. This is a picayune bit of a dissimilar indication, since it'due south beingness used more as a chronobiotic than a sleeping pill, merely the results were very similar: lower doses worked better than college doses. For example, in Lewy et al 2002, nightly doses of 0.5 mg worked to get a bullheaded subject field sleeping normally at night; doses of 20 mg didn't. They reasonably conclude that the twenty mg is such a high dose that it stays in their torso all day, defeating the point of a hormone whose job is to signal night. Other studies on the blind have generally confirmed that doses of effectually 0.3 to 0.5 mg are optimal.
There have been disappointingly few studies on sighted immature people. 1 such, Attenburrow et al 1996 finds that 1 mg works simply 0.3 mg doesn't, suggesting these people may need slightly higher doses, merely this study is a bit of an outlier. Another Zhdanova study on 25 year olds found both to piece of work equally. And Pires et al studying 22-24 year olds found that 0.3 mg worked amend than 1.0. I am less interested in judging the 0.3 mg vs. ane.0 mg debate than in pointing out that both numbers are much lower than the 3 – 10 mg doses institute in the melatonin tablets sold in drugstores.
UpToDate, the gold standard enquiry database used past doctors, agrees with these depression doses. "We advise the apply of low, physiologic doses (0.ane to 0.5 mg) for indisposition or jet lag (Grade 2B). High-dose preparations raise plasma melatonin concentrations to a supraphysiologic level and alter normal twenty-four hour period/dark melatonin rhythms." Mayo Clinic makes a like recommendation: they recommend 0.5 mg. John Hopkins' experts nigh agree: they say "less is more than" but end upwardly chickening out and recommending 1 to three mg, which is well above what the studies would advise.
Based on a bunch of studies that either favor the lower dose or bear witness no difference between doses, plus clear show that 0.3 mg produces an effect closest to natural melatonin spikes in salubrious people, plus UpToDate usually having the all-time recommendations, I'm in favor of the 0.3 mg number. I think you could make an argument for anything up to ane mg. Anything beyond that and you're definitely too high. Excess melatonin isn't grossly dangerous, simply tends to produce tolerance and might mess up your chronobiology in other ways. Based on anecdotal reports and the implausibility of becoming tolerant to a natural hormone at the dose you naturally accept information technology, I would judge sufficiently low doses are safe and effective long term, but this is only a judge, and nearly guidelines are cautious in saying anything after three months or so.
3. What are circadian rhythm disorders? How practice I employ melatonin for them?
Cyclic rhythm disorders are when your circadian rhythm doesn't match the normal wheel where you lot want to sleep at nighttime and wake up in the morn.
The well-nigh popular circadian rhythm disorder is "being a teenager". Teenagers' melatonin cycle is naturally shifted later, so that they don't want to go to bed until midnight or later, and don't want to wake up until eight or after. This is an obvious mismatch with school starting times, leading to teenagers either not getting enough sleep, or getting their sleep at times their body doesn't want to be asleep and isn't able to utilise it properly. This is why every reputable sleep scientist and relevant scientific body keeps telling the public school organization to start later.
When a this kind of tardily sleep schedule persists into adulthood or becomes too deplorable, nosotros call it Delayed Slumber Phase Disorder. People with DSPD don't get tired until very belatedly, and volition naturally sleep tardily if given the chance. The weak version of this is "beingness a nighttime owl" or "not beingness a forenoon person". The strong version just looks like indisposition: you go to bed at eleven PM, toss and turn until 2 AM, wake up when your alarm goes off at seven, and complain you lot "can't sleep". Merely if you can slumber at 2 AM, consistently, regardless of when you wake upwardly, and you would fall asleep as soon every bit your head hit the pillow if you first got into bed at ii, so this isn't insomnia – it's DSPD.
The opposite of this design is Advanced Sleep Phase Disorder. This is most common in the elderly, and I remember my grandfather having this. He would get tired around six PM, go to bed by 7, wake around 1 or 2 AM, and start his day feeling fresh and alert. But the weak version of this is the person who wakes up at 5 each morning fifty-fifty though their alarm doesn't go off until eight and they could really utilize the extra 2 hours' slumber. These people would probably do fine if they just went to bed at 8 or ix, just the demands of work and a social life make them feel like they "ought" to stay up as late as anybody else. So they become to bed at eleven, wake up at 5, and mutter of "terminal insomnia".
Finally, at that place'south Non-24-Hour-Sleep Disorder, where somehow your biological clock ended upward deeply and unshakeably convinced that days on World are 20-five (or whatever) hours long, and decides this is the colina it wants to die on. So if you lot naturally slumber eleven – seven one night, you'll naturally sleep 12 – 8 the next night, 1 to ix the nighttime later that, and so on until either you make a complete 24-hour cycle or (more likely) you go so tired and confused that you stay up 24+ hours and break the cycle. This is most common in blind people, who don't accept the visual cues they demand to remind themselves of the 24 hour twenty-four hours, but it happens in a few sighted people also; Eliezer Yudkowsky has written about his struggles with this condition.
Melatonin effectively treats these conditions, just you lot've got to utilise it right.
The general heuristic is that melatonin drags your sleep time towards the management of when you have the melatonin.
So if you want to become to sleep (and wake upward) earlier, you lot want to take melatonin early in the twenty-four hours. How early? Van Geijlswijk et al sums up the enquiry every bit saying it is about constructive "5 hours prior to both the traditionally determined [dim lite melatonin onset] (circadian time 9)". If you don't know your ain melatonin cycle, your best bet is to take it 9 hours later on you wake upwards (which is presumably near 7 hours earlier y'all become to slumber).
What if you want to go to slumber (and wake up) later? Our agreement of the melatonin cycle strongly suggests melatonin taken first matter upon waking up would work for this, but as far every bit I know this has never been formally investigated. The best I can detect is researchers saying that they think it would happen and beingness confused why no other researcher has investigated this.
And what nearly non-24-hour slumber disorders? I think the goal in treatment here is to accelerate your stage each day by taking melatonin at the same fourth dimension, then that your sleep schedule is more dependent on your own supplemental melatonin than your (screwed upwardly) natural melatonin. I see alien advice about how to do this, with some people proverb to apply melatonin as a hypnotic (ie simply before you go to bed) and others proverb to use it on a typical phase advance schedule (ie nine hours later waking and seven before sleeping, plausibly about 5 PM). I call back this 1 might exist complicated, and a qualified sleep doctor who understands your personal rhythm might be able to tell y'all which schedule is best for yous. Eliezer says the latter regimen had very impressive furnishings for him (search "Last but non to the lowest degree" here). I'thou interested in hearing from the MetaMed researcher who gave him that recommendation on how they knew he needed a phase advance schedule.
Does melatonin used this manner cause drowsiness (eg at 5 PM)? I call back it might, but probably such a minimal amount compared to the non-sleep-conduciveness of the hour that it doesn't register.
Melatonin isn't the only manner to accelerate or filibuster sleep phase. Here is a handy cheat canvas of research findings and theoretical predictions:
TO Care for DELAYED PHASE Sleep DISORDER (ie you lot get to bed too late and wake up too late, and yous desire it to be earlier)
– Accept melatonin nine hours later on wake and vii before sleep, eg 5 PM
– Cake blue light (eg with blue-blocker sunglasses or f.lux) later sunset
– Expose yourself to bright blue low-cal (sunlight if possible, dawn simulator or light boxes if not) early in the forenoon
– Get early morning time do
– Beta-blockers early in the morning (not generally recommended, but if you're taking beta-blockers, take them in the forenoon)
TO Treat ADVANCED PHASE SLEEP DISORDER (ie yous go to bed too early and wake up as well early, and you want it to be later)
– Accept melatonin immediately later on waking
– Block blue light (eg with blue-blocker sunglasses or f.lux) early on in the morning
– Expose yourself to brilliant blue lite (sunlight if possible, low-cal boxes if not) in the evening.
– Get tardily evening do
– Beta-blockers in the evening (non generally recommended, merely if you're taking beta-blockers, take them in the evening)
These don't "cure" the condition permanently; y'all accept to proceed doing them every day, or your circadian rhythm volition snap back to its natural pattern.
What is the right dose for these indications? Here in that location is a lot more controversy than the hypnotic dose. Of the 9 studies van Geijlswijk describes, vii have doses of five mg, which suggests this is something of a standard for this purpose. But the only study to compare unlike doses directly (Mundey et al 2005) found no difference between a 0.3 and 3.0 mg dose. The Cochrane Review on jet lag, which we'll encounter is the same procedure, similarly finds no difference betwixt 0.5 and 5.0.
Van Geijlswijk makes the important indicate that if you take 0.iii mg seven hours before bedtime, none of it is going to exist remaining in your system at bedtime, so information technology's unclear how this even works. But – well, information technology is pretty unclear how this works. In particular, I don't retrieve there's a great well-understood physiological explanation for how taking melatonin early in the day shifts your circadian rhythm vii hours after.
Then I think the show points to 0.3 mg being a pretty adept dose here as well, but I wouldn't blame y'all if you wanted to endeavor taking more.
4. How exercise I employ melatonin for jet lag?
Most studies say to take a dose of 0.3 mg only before (your new time zone'southward) bedtime.
This doesn't brand a lot of sense to me. It seems like you should be able to model jet lag as a circadian rhythm disorder. That is, if you move to a fourth dimension zone that'southward five hours earlier, y'all're in the exact same position as a teenager whose cyclic rhythm is set five hours after than the rest of the world's. This suggests you should utilise DSPD protocol of taking melatonin nine hours after waking / five hours before DLMO / seven hours earlier sleep.
My gauge is for nearly people, their new time zone bedtime is a couple of hours earlier their old bedtime, then you're getting most of the outcome, plus the hypnotic effect. But I'one thousand non sure. Mayhap taking information technology earlier would piece of work better. But given that the new light schedule is already working in your favor, I think almost people observe that taking information technology at bedtime is more than than good enough for them.
five. I try to use melatonin for sleep, only information technology simply gives me weird dreams and makes me wake up very early on
This is my experience also. When I use melatonin, I notice I wake the next morning with a jolt of energy. Although I usually have to grudgingly pull myself out of bed, melatonin makes me wake upwards bright-eyed, smiling, and ready to face up the day alee of me…
…at 4 AM, invariably. This is why despite my interest in this substance I never take melatonin myself anymore.
There are many people like me. What'south going on with us, and tin can we detect a way to make melatonin piece of work for us?
This bro-science site has an uncited theory. Melatonin is known to suppress cortisol production. And cortisol is inversely correlated with adrenaline. So if you lot're naturally very depression cortisol, melatonin spikes your adrenaline too high, producing the "wake with a jolt" phenomenon that I and another people experience. I like the style these people think. They empathize individual variability, their model is biologically plausible, and information technology makes sense. It's also probably wrong; it has too many steps, and nothing in biology is ever this elegant or sensible.
I think a more parsimonious theory would have to involve circadian rhythm in some style. Even an 0.3 mg dose of melatonin gives your body the accented maximum amount of melatonin it would ever have during a natural circadian cycle. So suppose I want to get to bed at xi, and have 0.3 mg melatonin. At present my body has a melatonin summit (usually associated with the very center of the nighttime, like three AM) at 11. If information technology assumes that ways it'due south actually 3 AM, then it might decide to wake up 5 hours subsequently, at what it thinks is eight AM, but which is actually 4.
I think I have a much weaker circadian rhythm than most people – at least, I take a lot of naps during the 24-hour interval, and fall asleep about equally well whenever. If that's true, maybe melatonin acts as a superstimulus for me. The normal tendency to wake up feeling refreshed and alert gets exaggerated into a sudden irresistable jolt of awakeness.
I don't know if this is any closer to the truth than the adrenaline theory, just information technology at least fits what nosotros know almost circadian rhythms. I'm going to endeavor to put some questions near melatonin response on the SSC survey this twelvemonth, and then start trying melatonin now so you can provide useful data.
What about the weird dreams?
From a HuffPo article:
Dr. Rafael Pelayo, a Stanford University professor of slumber medicine, said he doesn't think melatonin causes vivid dreams on its own. "Who takes melatonin? Someone who'due south having trouble sleeping. And once you have anything for your sleep, once you lot start sleeping more or amend, you lot have what'due south called 'REM rebound,'" he said.
This means your torso "catches up" on the slumber stage known as rapid eye movement, which is characterized by high levels of brain-wave activity.
Normal subjects who take melatonin supplements in the controlled setting of a sleep lab practice not spend more fourth dimension dreaming or in REM sleep, Pelayo added. This suggests that at that place is no inherent property of melatonin that leads to more than or weirder dreams.
Okay, but I usually take normal slumber. I take melatonin sometimes because I similar experimenting with psychotropic substances. And I still become some really weird dreams. A Slate announcer says he's been taking melatonin for 9 years and all the same gets crazy dreams.
We know that REM sleep is most mutual towards the end of sleep in the early morning. And we know that some parts of sleep structure are responsive to melatonin direct. At that place's a lot of debate over exactly what melatonin does to REM slumber, but given all the reports of altered dreaming, I call back you could pull together a case that information technology has some role in sleep compages that promotes or intensifies REM.
vi. Does this relate to any other psychiatric conditions?
Probably, but this is all still speculative.
Seasonal affective disorder is the clearest suspect. We know that the seasonal mood changes don't have annihilation to practise with temperature; they seem to be based entirely on wintertime having shorter (vs. summer having longer) days.
There's some show that there are two dissever kinds of winter depression. In one, the tardily sunrises train people to a late circadian rhythm and they terminate up phase-delayed. In the other, the early sunsets train people to an early circadian rhythm and they cease up phase-advanced. Plausibly SAD besides involves some combination of the two where the circadian rhythm doesn't know what information technology's doing. In either case, this can make sleep non-circadian-rhythm-congruent and and so less effective at doing whatever it is sleep does, which causes mood bug.
How does sunrise time touch on the boilerplate person, who is rarely awake for the sunrise anyway and ordinarily sleeps in a night room? I think your brain subconsciously "notices" the time of the dawn even if you are asleep. There are some weird pathways leading from the eyes to the nucleus governing circadian rhythm that seem contained of any other kind of vision; these might be keeping tabs on the sunrise if even a little exterior light is able to leak into your room. I'm basing this likewise on the claim that dawn simulators piece of work even if you lot sleep through them. I don't know if people get seasonal affective disorder if they sleep in a completely enclosed spot (eg underground) where at that place'due south no conceivable way for them to monitor sunrise times.
Bright calorie-free is the standard treatment for SAD for the aforementioned reason it's the standard handling for any other circadian phase delay, but shouldn't melatonin work likewise? Yes, and there are some preliminary studies (paper, commodity) showing it does. You accept to be a scrap conscientious, because some people are phase-delayed and others phase-advanced, and if you use melatonin the wrong manner it will make things worse. Simply for the standard phase-filibuster type of SAD, normal stage advancing melatonin protocol seems to go well with bright calorie-free as an boosted handling.
This model also explains the otherwise disruptive trend of some Deplorable sufferers to get depressed in the summer. The problem isn't amount of light, it'south circadian rhythm disruption – which summertime can do just also equally winter can.
I'm also very suspicious there'southward a strong cyclic component to depression, based on a few lines of prove.
First, one of the most classic symptoms of depression is awakening in the very early on morning and not being able to get back to sleep. This is confusing for depressed people, who usually call up of themselves as very tired and needing to slumber more than, but it definitely happens. This fits the contour for a circadian rhythm result.
Second, agomelatine, a melatonin counterpart, is an effective (ish) antidepressant.
Third, for some reason staying awake for 24+ hours is a very constructive depression treatment (admitting temporary; y'all'll go back to normal after sleeping). This seems to sort of be a way of telling your cyclic rhythm "Yous tin can't fire me, I quit", and at that place are some complicated slumber deprivation / cyclic shift protocols that try to leverage it into a longer-lasting cure. I don't know anything about this, but it seems pretty interesting.
Fourth, nosotros checked and depressed people definitely accept weird circadian rhythms.
Last of all, bipolar has a very strong cyclic component. There aren't a whole lot of lifestyle changes that really work for preventing bipolar mood episodes, only one of the big ones is keeping a steady bed and wake time. Social rhythms therapy, a rare effective psychotherapy for bipolar disorder, revolves around training bipolar people to control their cyclic rhythms.
Theories of why circadian rhythms matter and then much revolve either effectually the idea of pro-circadian slumber – that sleep is more restorative and effective when it matches the cyclic cycle – or the thought of multiple circadian rhythms, with the torso functioning meliorate when all of them are in sync.
7. How can I know what the best melatonin supplement is?
Labdoor has done purity tests on various brands and has ranked them for yous. All the ones they highlight are yet ten to thirty times the advisable dose (also, stop calling them things like "Triple Force!" You don't want your medications to exist likewise strong!). As usual, I trust NootropicsDepot for things like this – and sure enough their melatonin (available on Amazon) is exactly 0.three mg. God bless them.
Source: https://slatestarcodex.com/2018/07/10/melatonin-much-more-than-you-wanted-to-know/
0 Response to "Can I Give My 1 Year Old Melatonin"
Post a Comment